I remember distinctly the day that changed the way I thought and changed my life’s mission into the direction I’ve taken over the past decade.
It was March 2, 2004 in Iraq – a day that was pivotal for me and really drove my mission in healthcare. I was in Bagdad; it was a hot day, and it was a religious holiday. It was Ashura, the most important holy day on the Shiite Muslim calendar. There were thousands of people marching on the road. They were the faithful, the hopeful, the committed – they’re marching on this religious holiday, and mingled in with that crowd were suicide bombers. They detonated themselves. All of a sudden, this peaceful, religious observance turned into a scene of complete chaos.
Dr. Sudip Bose and his team work on an injured soldier in Iraq.
Suddenly there were dozens and dozens of injured lying all over the place. Smoke and dust from the explosions drifted through the air. Screams rang out from all along the road. I was the only physician anywhere near the scene, somewhere around 800 meters away from the area of the detonations. Our team rushed into the middle of it all, and at that moment, immersed in the chaos, everything went into slow motion. I looked around, and I was wondering, how am I going to address all these patients? How am I going to get to everyone and see everyone and help everyone? It was an overwhelming thought.
But in slow motion, in my mind, I saw our medics moving into action. They were functioning autonomously. They were tying tourniquets, they were starting airway devices, they were patching up holes in chests, and at that moment, I was very grateful that we had taken the time to train those medics. Because by training those medics, I had multiplied myself. One physician can’t reach all these patients, but by training the medics, I had multiplied myself and we were able to address those casualties.
Dr. Sudip Bose (foreground, right) talks with a first-responder in the Emergency Department.
By Dr. Sudip Bose, MD, FACEP, FAAEM
You’ve likely heard the term “single-payer” used during the course of discussions of how to solve the problems America is having in ironing out a healthcare system that works for all the people.
I’ve had some experience in a single-payer system of healthcare – the US military. I trained and worked in single-payer for over a decade when I was an Army doctor. I was both patient and provider. And I’ve got one thing to say about it: Don’t be disillusioned. Single-payer is not something that will solve all our healthcare concerns. It’s one option being discussed, but it’s not the golden ticket, if you will. Nothing is, actually. It certainly has its advantages, but there also are disadvantages that the American public may not like. There are good things and bad things about almost any healthcare proposal. It seems to me that in America, we’re at a crossroads of looking for the lesser of evils when it comes to healthcare.
So let’s look at the good, the bad and the ugly as it relates to a single-payer system.
THE GOOD
Let’s start out by defining what single-payer healthcare is. This explanation that you can find on Wikipedia seems as good as any:
Dr. Sudip Bose spins his laptop on his finger as if it’s pizza dough while making a point at a recent speaking engagement.
By Dr. Sudip Bose, MD, FACEP, FAAEM
It’s been said that the one thing that people fear more than death is speaking in public. I was struck by comedian Jerry Seinfeld’s observation on that. He said, in effect, that more people attending the memorial service would rather be in the casket than delivering a eulogy at the podium in front of the gathered crowd. Interesting observation, right?
Sure, public speaking can be intimidating. You’re up there, out front, all alone, your words echoing around the venue, sometimes with very little reaction. Are you hated? Are you liked? Are you loved? Is anyone even paying attention to you? All those thoughts flash through your mind as you search the crowd in front of you for a face that seems sympathetic. You hope the person you lock in on as that person with the seemingly sympathetic-looking face isn’t merely trying to abstain from passing gas and has his own worries in mind.
Will your jokes ring hollow, or will you get a reaction? Will your brief demo of spinning a laptop on your finger tip like you would do with pizza dough be a source of rousing recognition and perhaps even applause?
It can be tough to be a speaker in a public arena. But I’ve found by keeping the acronym CHIPS in mind, you can master public speaking. Let me go through each letter of the acronym and explain:
C is for Confidence
This is an absolute must. You must be confident. You must be sure of your subject and your ability to deliver and communicate the information you are speaking on effectively to your audience.
It’s amazing how an audience can sense fear. And it’s amazing how quickly a talk can unravel if you don’t have confidence in your delivery of information. Sure, almost everyone is nervous when walking on stage or a lectern to deliver a speech in front of dozens, hundreds or thousands. Performers at the top of their game who are wildly popular sometimes have literally gotten physically ill before they went on stage. The singer Lorde, for example, who burst onto the scene with her hit “Royals” said in an interview that she has thrown up before her show. “I am reduced by nerves,” the singer said. “I can be completely crushed by feelings of all kinds … I get nervous, I get freaked out …”
Other celebrities with stage fright include the singers Rod Stewart and Barbara Streisand (who dodged performing for years because of it), actor Mel Gibson, and comedienne Carol Burnett (who reportedly threw-up before many of her performances).
Yet they gathered themselves up, shoved their fear into a virtual closet, shut it away and went on to do their work with confidence. It’s the only way. You must project confidence in front of an audience. That said, it’s not the end of the world if you don’t; everyone has a bad day every now and then. But to be an effective public speaker, having confidence leads the list of attributes you want to have.
TJ Walker is a public speaking expert and has this to say about the importance of speaking with confidence: How to Speak With Confidence.
H is for Humility
Remember, I said confidence, not arrogance. There’s a difference. You must work to convey a sense of humility when you’re in front of people and not come off as being an arrogant a… Well, you know. There can be a fine line between confidence and arrogance.
Don’t think you can just wing it – at least not at first. Don’t be that arrogant person who thinks he or she can just jot down a few notes the night before, get out on stage and give a masterful performance. If you can do that, you’d be one of the very few. More often than not, you’ll let yourself and your audience down. Arrogance can lead to your undoing.
Why humility, though? After all, you’re speaking to a group for a reason. You’re a leader in your field and recognized as such or you wouldn’t have gotten the speaking engagement in the first place. But you’ve got to be able to show that you’re serving something beyond your own interests – perhaps there’s something you struggled with in the past and had to overcome. Sharing an experience like that creates empathy, shows humility in exposing a vulnerability, and helps make a connection with your audience.
Quite often as human beings, we connect with each other through struggle – shared in real time, or shared with an audience after the fact. When you connect with others through struggle, you’re communicating with your audience in a way that shows that you and they are on an equal level in that regard. They think, “I’ve had to deal with that, too.” Or, “I’ve felt that way, too.” Or, “I know how that feels.”
Tony Robbins, perhaps currently one of the top public speakers, says that, “The way to move an audience is by becoming moved yourself, which can only happen if you’re being genuine.” And, he says, “You need to be in the moment and flexible to make it real and raw. You’ll enjoy it, they’ll enjoy it, and you’ll be memorable.”
It’s a delicate balance – showing confidence and humility at the same time – but one you should strive for when speaking to an audience.
I is for Inspiration
Speak to serve. Speak to inspire. Public speaking is not about you, it’s about your audience. You’re giving the talk, theoretically, to benefit your audience and to communicate your life experience to provide, hopefully, a different way of looking at things. You’re there to hopefully connect with the listeners. Inspire them as best you can; give them a different perspective; allow them to access your experience, your learning, your development, to motivate, and hopefully along the way, to entertain.
Focus on inspiring your audience, and that can also help you with your confidence, because it takes the pressure off your self-consciousness and introspection and places the focus on your audience and flips the speaking process into a mode of being an extroverted speaker with the listeners placed in the spotlight. That’s what I try to do when I talk, and I try to focus on the following goals to hopefully benefit the audience:
Teach executives leadership tactics in crisis situations
Develop quality leaders with integrity in an organization
Improve decision making to increase company sales
Enhance communication strategies to better engage employees
Train, inspire and motivate
Keep the audience laughing, learning and energized
Raise funds and awareness for injured combat veterans
In the preparation work I do leading up to my presentation, I keep those goals – my purpose in speaking – in mind. I think, “How can I help the audience achieve their goals? It’s an outward focus rather than inward focus.
You can’t prepare for a talk enough. Practice, practice, practice. Don’t just write your presentation, give it. Talk to the furniture in your house. Have your husband, wife, son, daughter, friend, stranger – whomever – listen to you give your speech. Stand in front of a mirror and give your talk. Videotape yourself and play it back while watching with a critical eye.
Revise, redo and keep trying to find that presentation sweet spot. The more you practice, the more comfortable you’ll feel during your talk. When you feel like your speech is as familiar as that comfortable, well-worn flannel shirt you own, you know you’re at the right spot.
Speech, as in speaking, as in using your voice effectively – as in using your voice as a tool to connect with your audience. Understand the effective use of your voice. As part of your preparation, you must learn how to speak with effective modulation, tone, pacing and … the proper use of pausing for effect.
One of the most effective speakers I’ve ever heard was Jim Rohn. He had such a way of modulating his voice for effect and throwing in very calculated pauses in some very unusual ways and in unexpected places as he spoke. His voice rose, almost in question; it dropped very low when making a point; it paused often, to great effect.
It’s very hard to write about it, but you certainly can hear him and perhaps better understand what I mean by checking out this video of him speaking. This is a great talk on the need to have discipline in your life:
You can use the links that populate with that video to springboard to other links of him speaking. Listen to how he modulates his voice, how he slows down his words, then speeds them up, almost staccato-like. Pay attention to the pauses he places in his talk – very effectively. Listen to him repeat his key points.
Remember to repeat. And repeat often to drive home key points. There’s so much you can learn from listening to great speakers.
As far as my speaking engagements go, here’s a clip that contains a compilation of a handful of appearances I’ve made: Keynote Speaker: Dr. Sudip Bose.
I enjoy giving back and educating others. I frequently speak at corporations and take the skills I learned in combat and in the emergency room to teach leadership lessons and how to apply them to everyday life – it’s probably my favorite topic to speak on. Through my lectures and media appearances throughout the country, I’m able to raise awareness and funds for TheBattleContinues.org. The Battle Continues Inc. is a 501(c)(3) nonprofit organization aimed to raise awareness and help veterans who have returned from war; 100 percent of money donated to the organization goes towards assisting and supporting veterans. I also promote healthy living and awareness on health care issues so that people can make better-informed decisions regarding their health. I’m a firm believer that our health is our single most important asset.
So remember the acronym “CHIPS” when it comes to public speaking; and remember, as my motto proclaims, to “keep your inner Army strong.”
To learn more about Dr. Sudip Bose, MD, please go to SudipBose.com and visit his nonprofit TheBattleContinues.org where 100 percent of donations go directly to injured veterans.
Getting shot at tends to get you focused very quickly and very specifically on what you need to do to take control and eliminate the threat. I mean that literally; I learned that on the battlefields of Iraq. It’s the kind of thing that creates instant leadership. You figure out how to overcome the problem in front of you, or you very possibly will die.
In the medical arena, when I was an intern, I faced my first “code” patient. “Code” is doctor talk for cardiopulmonary arrest – a heart stopping – in a patient in a hospital. When that happens, there are codes associated with each patient that determine the level of response by a medical code team – all the way from a full code, where every effort is made to resuscitate someone, to a limited code, to a “DNR,” or Do Not Resuscitate. A code team of medical professionals will rush to the patient and immediately begin appropriate medical treatment. On my first code response, I rushed into the room and froze. I didn’t really know what to do. And I remember the eyes on me, watching my inaction. I knew from that day on, that I needed to know what was going on. I learned that if I was going to be a leader, I had a need to learn what to do when I come face to face with a pulseless patient. Because when a patient codes, you need to take control, and you need to act quickly and decisively. You need to lead. I needed to learn fast, and I needed to continue to learn.
Diversity
At no other time on earth has the pace of change been so rapid. At no other time in history have leaders had to understand and process so much information to arrive at a decision. Also, at no other time have such diverse generations been in the work force – Baby Boomers, Generation Xers, Millenials – and they each have such a diverse work ethic and a divergent sense of reward.
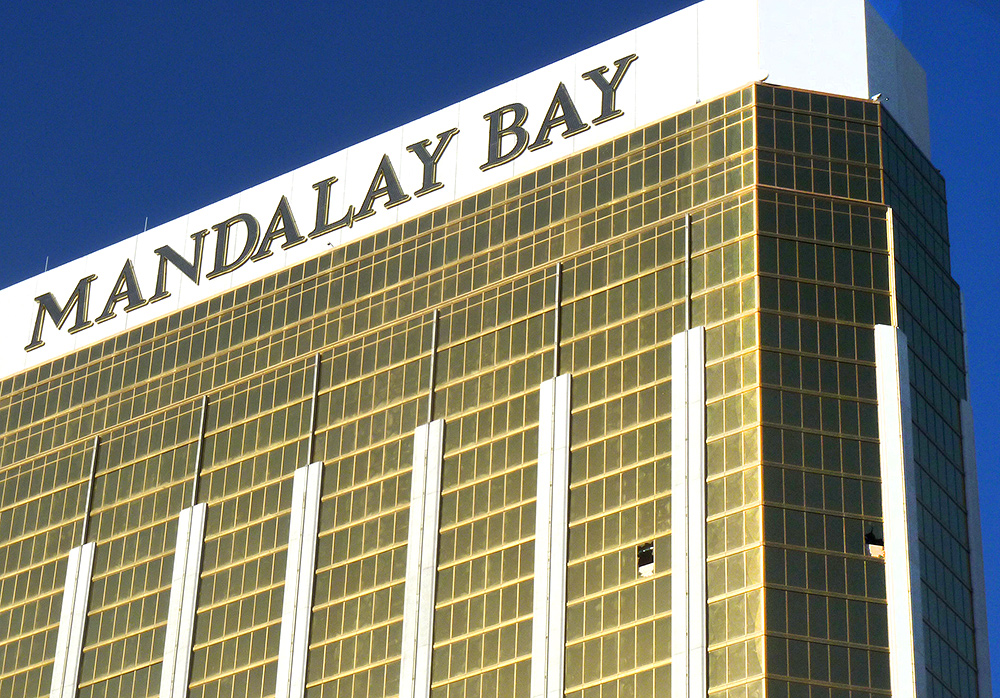
Broken-out windows (lower right in image) on the 32nd floor of Mandalay Bay Resort and Casino on Las Vegas Boulevard from which a shooter rained bullets down on innocent concert-goers, killing 58 and injuring nearly 500.
By Dr. Sudip Bose, MD, FACEP, FAAEM
“The worst act imaginable often brings out the best of people.”
You’ve likely heard that phrase, probably often repeated, during the news coverage of the horrific mass shooting at the Route 91 Harvest Festival outdoor concert on the Strip in Las Vegas on Sunday, Oct. 1, as well as during the aftermath of hurricanes Harvey, Irma and Maria.
As a physician and especially as an emergency department doctor, we train for mass casualty situations on a routine basis, always hoping we never have to experience such an incident in reality. It’s a concept I accepted as a medical officer on the front lines of Iraq in the Army: We prepare in peacetime for wartime. When a mass casualty situation happens, that’s exactly what it’s like – you get thrust into a war zone immediately.
And it takes an Army to carry out the mission needed to try to keep casualties as low as possible.
At 10:05 pm Sunday night, shots rang out from the upper floors of the Mandalay Bay Resort and Casino on Las Vegas Boulevard. Initially most people thought what they heard might be fireworks associated with the concert. But all too soon, concert-goers realized that they were being fired upon as hundreds of rounds of bullets rained down on them. It didn’t take long for that “Army” to swing into action on the ground to start treating the wounded. First responders, as well as concert-goers themselves, immediately started do what they could to stop the bleeding of those hit. They had to get the injured stabilized and transported to hospitals. Las Vegas area hospital emergency departments quickly became saturated with patients. Victims – 5, 6, 7, 8 at a time – were piled into ambulances at the scene of the shooting and rushed away for treatment. Eyewitnesses to the shooting event also reported that gunshot victims were loaded into pickup trucks and civilian cars in some cases and transported to hospitals.
First there was Harvey, then Irma and, most recently, Maria. Hurricanes have hit Texas and the Gulf Coast, have torn through Florida, and have raked across the Caribbean, devastating Puerto Rico and the Virgin Islands. These disastrous power punches have left scores dead, millions uprooted and much physical and emotional devastation in their wake.
How can that happen, you ask? Shouldn’t these kinds of victims have been our top priorities for keeping safe? Of course. But sometimes, all the planning and precaution in the world can’t overcome the unpredictability of Mother Nature, a disabled infrastructure and the failure of emergency backup power.
Every natural disaster, such as hurricanes Harvey, Irma and Maria, also becomes a looming public health disaster. As the storms approach, each hospital, nursing home and medical facility that houses patients must make difficult decisions between evacuating patients and staff and battening down to ride out the storm. Evacuations pose major logistical issues as patients, staff, equipment and medications all have to be transitioned from one location to another. An evacuation for a chronically or critically ill patient can be life-threatening. During the height of the storms, hospitals and other medical facilities face critical issues in trying to keep their patients not only alive, but also well cared for. Shortages of food, water, medicine and power can turn very bad very quickly.
After the Storm
After the brunt of hurricanes like Harvey, Irma and Maria push through, health resources re-focus on fighting infections, both from bacteria in floodwaters and from mosquitoes. Physicians scramble to contain potential epidemics that might arise after flooding. Based on the health problems that arose after Hurricane Katrina, medical professionals have to prepare to try to avert major public-health emergencies, environmental illnesses, and outbreaks, which could intensify in the aftermath of the devastating blows dealt by these hurricanes. Sewage that has overflowed its containment can pose a major health issue, as can spilled fuel and chemicals from tanks and pipelines torn apart during the hurricanes.
And not only that, but for hospitals and other facilities that made the decision to move patients, those same patients have to be transitioned back home to their original facilities at some point, assuming those facilities are able to open and operate again.
As you can see, there is much to consider when preparing for a natural disaster like hurricanes Harvey, Irma and Maria. In fact, the Centers for Medicare and Medicaid Services have established an Emergency Preparedness Rule that all hospitals and health care facilities must have a plan in place and be in compliance by Nov. 16, 2017. This emergency preparedness plan, by CMS guidelines, must address an all-hazards risk assessment and contain four core elements:
Four Core Elements of Emergency Preparedness RISK ASSESSMENT AND EMERGENCY PLANNING (include but not limited to):
Hazards likely in geographic area
Care-related emergencies
Equipment and power failures
Interruption in communications, including cyber attacks
Loss of all/portion of facility
Loss of all/portion of supplies
Plan is to be reviewed and updated at least annually
COMMUNICATION PLAN
Complies with federal and state laws
System to contact staff, including patients’ physicians, other necessary persons
Well-coordinated within the facility, across health care providers, and with state and local public health departments and emergency management agencies.
POLICIES AND PROCEDURES
Complies with federal and state laws
TRAINING AND TESTING
Complies with federal and state laws
Maintain and at a minimum update annually
The plan must also consider those individuals locally who may be deemed “at risk.” To quote from the CMS guidelines:
“At-risk populations are individuals who may need additional response assistance, including … [those] from diverse cultures, [who] have limited English proficiency, or are non-English speaking.”
In addition to shelters, hospitals are often a focal point of their communities during a crisis. In addition to patients already admitted to a hospital, during a natural disaster like a hurricane, new patients are very likely to seek medical assistance by coming to the emergency department either on their own or after being rescued by a first responder. And first responders need to know the status of a hospital to ensure they’re transporting patients to an open, operating, safe medical facility. Hospitals need to work with other hospitals to know where to send or receive patients if any of the open facilities become overwhelmed. And as always, hospitals need to remain HIPAA-compliant regarding patient information; just because a hospital might be operating within a disaster doesn’t mean it can be casual or careless with personal patient information.
Once hurricanes like Harvey, Irma and Maria have passed and done their damage, the next challenge is keeping the most critically ill patients cared for. We’re seeing that now, and especially so, in Puerto Rico, which is an island. You just can’t drive trucks there loaded with food, fuel, water and medical supplies. All that has to be flown in or shipped in.
Finding Comfort
“The other challenge that we face, is unfortunately because of the severity of the hit [from Hurricane Maria] there is diminished capacity of local governments and state government to respond similar to what we saw with Texas and Florida,” said Brock Long, FEMA Administrator. “So therefore, it is requiring us to push forward a lot of resources, including the USS [sic] Comfort, which is on the way.”
The USNS Comfort is a Navy hospital ship that sails to points of distress when needed to assist medical personnel on the ground with there most dire patients and circumstances. It is heading to Puerto Rico. It has one of the largest trauma facilities in the United States. It has a supply of 5,000 units of blood, according to a U.S. Navy fact sheet about the vessel, and is equipped with a full spectrum of surgical and medical services including X-ray machines, CAT scan units, a dental office, an optometry facility, a physical therapy center and a pharmacy. The 1,000-bed ship was sent to Haiti in 2010 after a large earthquake killed upwards of 300,000 people. In 2005, the ship sailed to the Gulf Coast after Hurricane Katrina hit and more than 1,500 people were treated aboard the vessel. In 2003, the hospital ship spent two months in the Persian Gulf during the invasion of Iraq, and it also was deployed to New York in the aftermath of 9-11.
Getting medical support to areas ravaged by these hurricanes and other natural disasters can be formidable. The news media may leave these areas after the initial news is reported and the days march on; however, the support needed for medical personnel, supplies and treatment carries on for months until the area stabilizes.
Right now in Puerto Rico, according to a report by Reuters, “For hospitals across this region, the challenges are mounting. After the power went out, back-up generators at some hospitals failed quickly. Other hospitals are running critically low on diesel. Fuel is so precious that deliveries are made by armed guards to prevent looting, according to Dr. Ivan Gonzalez Cancel, a cardiovascular surgeon and director of the heart transplant program at Centro Cardiovascular,” the report said.
People line up for blocks trying to get enough fuel to power generators and vehicles, waiting for sometimes up to seven hours. Everything else there is in a shambles as well, adding to the urgency and stress. Food is scarce. The island’s electrical grid has gone down and may stay that way for months.
“Cellular service, internet, and email have virtually disappeared, hurling a modern society into a bygone era,” Reuters reported. “Radio has become a primary source of information.”
For hospitals that need to transfer critical patients because they can’t support them due to lack of electricity, the situation is dire. For them, the USNS Comfort can’t arrive fast enough. If necessary, the most critical patients can be evacuated via medevac and transferred to the USNS Comfort while it’s still underway and sailing towards Puerto Rico.
And in the meantime, if medical staff on the island can’t get gasoline for their cars, how can they even get to work to care for the sick and injured?
FEMA’s Twitter feed has been carrying photos of ongoing efforts in Puerto Rico: The American Red Cross is on the scene, as is the Salvation Army, U.S. state urban search and rescue teams, the National Guard, Customs and Border Protection is assisting, the U.S. Coast Guard, the U.S. Navy, Veterans Administration medical centers are supporting by taking in evacuated patients … it goes on and on. The effort is just massive and won’t end anytime soon. (Also see, The Guardian: Photos After Hurricane Maria)
Getting Help
All these areas – Texas with Hurricane Harvey, Florida with Hurricane Irma, and Puerto Rico with Hurricane Maria – need our continued help and support on a variety of fronts. And we also should not forget those suffering in Mexico, which was hit recently with major earthquakes resulting in a death toll of at least 333 people and counting. Here are some links and suggestions for ways you can donate, if you are moved to do so, culled from relief websites and media:
Those are just a handful of entry points for support and donations and sources for helping victims. Use your discretion for any donation should you decide to help out. Let’s hope these areas get the continued support they desperately need.
To learn more about Dr. Sudip Bose, MD, please go to SudipBose.com and visit his nonprofit TheBattleContinues.org where 100 percent of donations go directly to injured veterans.
Veterans wrote a blank check on their lives when they volunteered to join the military, went to war in many cases, and risked not coming home to their families. Some never got to see their children be born because they were overseas protecting our freedom. They truly did serve our country by giving up their normal lives for a life spent on guard, on watch, ready to fight and die, if necessary to protect Americans and keep our enemies at bay.
But what many people who haven’t served in the military don’t really understand, is that after veterans stop fighting the enemy, they continue the struggle fighting against injuries or illness sustained while on active duty – either physical or mental, or both. In many instances, their battle continues.
I know, because I’ve been there. I walked that walk. I was an officer in the Army and attained the rank of major; I served as a front-line physician in the Second Battle of Fallujah and served one of the longest combat tours by a physician since World War II, for which I earned the Bronze Star. I became an emergency physician while I was in the Army, and I now serve as an emergency room physician and also have become one of America’s most experienced doctors on mass casualties, disaster care and PTSD (Post-Traumatic Stress Disorder). I also created TheBattleContinues.org, which is a 501c(3) nonprofit entity aimed to raise awareness of veterans’ issues and help veterans who have returned from war. Every penny of the money donated to TheBattleContinues.org goes directly to the benefit of veterans.
The health challenges veterans face are unique, almost entirely unlike those faced by any other demographic in America. A Washington Post / Kaiser Family Foundation poll taken in 2013 showed that more than half of the service members polled who served in Iraq and/or Afghanistan admitted to suffering a physical or mental health problem as a result of their service. More service members than ever before have survived combat wounds that would have been fatal in previous wars. It’s now our responsibility as a nation to tend to our veterans when they return from overseas and are discharged from military service. Some of the things our veterans have to deal with include:
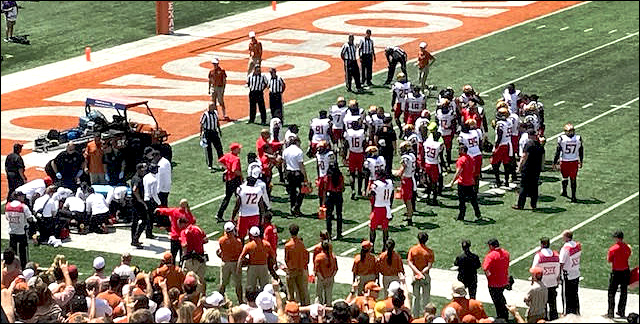
Medical and support personnel gather around Maryland cornerback Antwaine Richardson (left) as teammates wait for a sign that he’s OK.
By Dr. Sudip Bose, MD, FACEP, FAAEM
Football season has begun again, and already concussions have made news. This past Saturday during Labor Day weekend, the opening weekend for most college football teams, I happened to be at the University of Texas game against the University of Maryland. I was reminded, as was everyone watching the game at the stadium or elsewhere, just how violent the sport can be. A Maryland player sustained a head injury in the third quarter while trying to make a tackle. It knocked him out of the game.
Maryland cornerback Antwaine Richardson, a sophomore from Delray Beach, Florida, had to be carted off the field after a collision with Texas’ Lil’Jordan Humphrey. Richardson, who had already recorded six solo tackles in the game, suffered a head injury and lay motionless on the field for several minutes. He was eventually carted off the field and taken to a hospital, where he was responsive and moving, according to a Maryland spokesman who reported back. Richardson currently is in concussion protocol ― as he should be ― is listed as day-to-day, and is out for an undisclosed amount of time.
Maryland’s second-year coach, DJ Durkin, while happy about getting the program’s first win over a Top 25 team in seven years, had a decidedly serious tone at his news conference Tuesday when he confirmed just how severe several injuries were that were suffered not only by Richardson, but by quarterback Tyrrell Pigrome and linebacker Jesse Aniebonam. Durkin said that quarterback Pigrome would miss the rest of the season with a torn ACL of his right knee and that Aniebonam will be out “several months” with a fractured ankle.
“Unfortunately, injuries are part of our game, and they happen,” Durkin said at his news conference.
Spending on prescription medications is higher in the US, per capita, than in any other country in the world, according to a recent Journal of the American Medical Association study. And, the report said, those costs are “largely driven by brand-name drug prices that have been increasing in recent years at rates far beyond the consumer price index.”
An NBC News report noted that, “Paying for medicine can be the most expensive out-of-pocket health cost for Americans.”
Why?
If you look at the landscape of prescription drugs in America, you’ll notice there is nothing in place to keep drug prices low. There are no specific regulations to keep a ceiling on costs. The pharmaceutical manufacturers have the very tempting opportunity to charge whatever they think a drug’s demand and the market will bear. It’s simply possible for a drug company to charge high prices if they want to, just because they can. There’s nothing regulating whatever cost they want to charge. So the opportunity to charge more exists.
Drug companies will tell you immediately that their costs to research, develop and bring a drug to market are astronomical, and they have to cover those costs and make a profit to continue to stay in business and develop even more innovative prescription medications that will help save more lives. That’s a primary reason pharmaceutical companies will point to as a reason for escalating prices on all the medications they manufacture. And that’s true – to a degree.
“The opioid crisis is an emergency, and I’m saying officially right now it is an emergency. It’s a national emergency. We’re going to spend a lot of time, a lot of effort and a lot of money on the opioid crisis,” President Donald Trump said yesterday.
It’s likely that President Trump was influenced by an interim report that was presented to him last week by the Commission on Combating Drug Addition and the Opioid Crisis, which compared the nation’s overdose death toll to the toll that resulted from the terrorist attacks on 9-11: “With approximately 142 Americans dying every day, America is enduring a death toll equal to September 11th every three weeks,” the commission’s interim report noted. And the commission urged the president to declare a national emergency under either the Public Health Service Act or the Stafford Act.
President Trump and the commission are right in placing such an emphasis on this national crisis – and it is a national crisis. It’s the biggest epidemic to have hit our country since the HIV epidemic of years ago, so much so that in the emergency room as an emergency physician, I’m seeing patients come in dead from opioid overdoses. People are getting addicted and are coming into our emergency rooms and they’re dying from this. A couple of those instances I remember very vividly – one where a young girl went downstairs at her house to find her older brother and his girlfriend blue and not breathing; in another case a man looked out of the window of his house and saw a teenager lying still on his lawn. I know the stories, because the brother, the girlfriend and the teen on the lawn all came through my emergency room and all were dead from overdosing on opioids. You don’t forget those kinds of things.