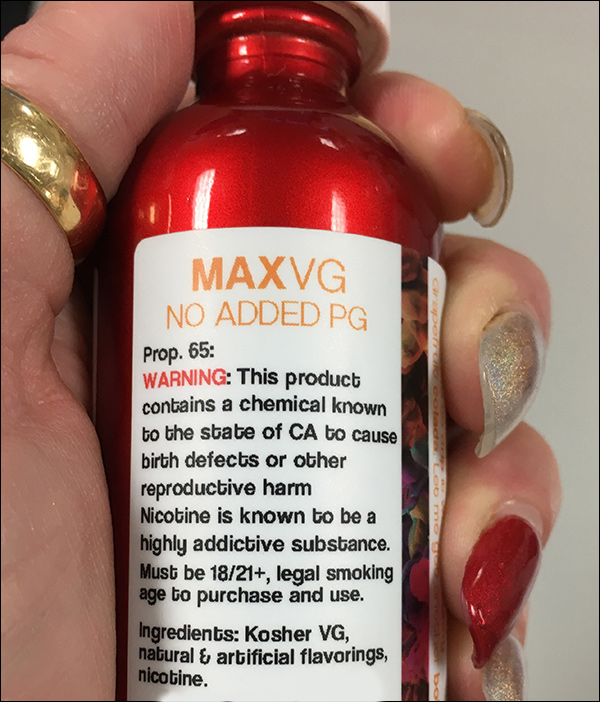
It is well known that cigarette smoking is dangerous to one’s health and to the health of others. For some, using e-cigarettes or “vapes” has allowed them to reduce or quit the use of tobacco. I applaud those who have been able to quit smoking by using these devices. It is a step in the right direction. However, as a practicing emergency room physician, I still have some concerns about the safety of these devices. As a friend who vapes once directly, albeit somewhat inelegantly, put it, “Only a moron would believe that inhaling [stuff] into your lungs is totally harmless.”
For the sake of this article, I will use the general term ENDS (electronic nicotine delivery systems), though I acknowledge that not all e-liquids contain nicotine. This is not an attack on people who use the devices or even sell them, but simply an attempt to educate Americans on the possible risks associated with their use. For the record: I absolutely am not incentivized by any pharmaceutical companies, government agency, political organizations or anyone else.
The Royal College of Physicians published research in the Annals of Internal Medicine and actually encouraged the use of ENDS. That may be misleading, however, because the study didn’t show that vaporizers and e-cigarettes are safe, but rather that their use is safer than smoking tobacco cigarettes. It is encouraging to note, however, that they do not think vaping is a gateway to cigarette smoking. This is especially important because of the popularity of ENDS use among younger people.
President Trump announced via Twitter last week in a series of three Tweets that United States government would no longer accept or allow transgender individuals to serve “in any capacity” as the military “cannot be burdened with the tremendous medical costs and disruption that transgender in the military would entail.” His three Tweets compiled:
“After consultation with my Generals and military experts, please be advised that the United States Government will not accept or allow transgender individuals to serve in any capacity in the U.S. Military. Our military must be focused on decisive and overwhelming victory and cannot be burdened with the tremendous medical costs and disruption that transgender in the military would entail. Thank you”
@realDonaldTrump
That’s quite a stance President Trump has taken, and a change to the military’s current policy of allowing gay, lesbian and bisexual people to serve openly after President Bill Clinton opened the door with his implementation of a “don’t ask, don’t tell” policy beginning in 1993 when it came to sexual preference/orientation in the military. The debate on this issue has gone back and forth over the past seven decades. Even as far back as World War II, those policies were the subject of substantial debate as the military eventually brought in some 18 million men over the course of that war. One of the “deviations,” as it was termed then, that physicians giving physicals to incoming soldiers joining to fight in WWII were asked to look for was listed as “homosexual proclivities,” which would disqualify someone trying to enter the military. Various administrations wrestled with the subject over the next five decades with the result being that of exclusion throughout the armed forces, until 1993, when Congress passed and President Clinton signed a law instituting the policy commonly referred to as “don’t ask, don’t tell” (DADT), which allowed gay, lesbian, and bisexual people to serve as long as they did not reveal their sexual orientation.
Then in 2010, the ban on openly gay, lesbian, and bisexual service personnel was ruled by two federal courts as being unconstitutional, and a federal appeals court suspended the DADT policy. In December 2010, Congress passed and President Barack Obama signed the Don’t Ask, Don’t Tell Repeal Act of 2010 and, under its provisions, restrictions on service by gay, lesbian, and bisexual personnel ended as of Sept. 20, 2011. Transgender people were allowed to openly serve starting June 30, 2016.
Now, let’s remember, this recent discussion was started by a Tweet from President Trump. And a Tweet is not an official directive. A day after the president Tweeted about transgenders in the military, Joint Chiefs of Staff Chairman, Gen. Joseph Dunford, announced that the current policy – meaning that policy set in place over a year ago regarding transgender people being allowed to openly serve in the military – will remain intact until the president issues an official directive.
Since that set of Tweets, there has been quite a bit of back-and-forth on both sides of the issue. Much of the discussion has been around a couple of things:
The medical costs of being transgender and maintaining a transgender status in the military and,
That the armed services should not be a place of implementing progressive social engineering and that the military should not have its readiness impacted by transgenders.
I have experience on the medical side of things as well as military (Dr. Sudip Bose’s profile). As far as the medical side of things go, most transgender patients do not undergo sexual reassignment surgery, which is expensive, has risks, and has a long timeline. Patients do have cosmetic surgeries to help assume a more masculine or feminine appearance, depending on the transformation aesthetics they’re looking for. Hormone therapy is common.
Also, making a transition from one gender identity to another is not just about a physical, outward appearance. That’s important to understand. Transitioning to become a man or a woman is an important part of a patient’s identity. A vast number of transgender people see themselves as, and identify themselves with being a male or female – opposite of the way they were born – at a very young age, often as children. For example, that “tomboy” girl who always wanted to play with the boys and associated with more traditionally masculine activities and possessions; then there’s the young boy who always wanted to play with the girls and befriend them, who felt more comfortable in his own identity playing with dolls or wearing a dress – typically more traditionally feminine behavior.
Becoming a transgender person is a long and complicated process for an individual. Some people may modify the way they look and dress and become more feminine or masculine in appearance and may even change their name before doing it legally. Some transgenders will make the transition in only part of their lives, for example assuming a male or female persona personally, while at home, but may remain the opposite gender at work. There are those who have come into the emergency department and present themselves as their original birth gender, despite having made the transition to the opposite sex in every other aspect of their lives.
However a transgender person presents him or herself – male or female –however they identify themselves, regardless of what you might initially perceive them to be, is the way they need to be treated. It’s actually pretty simple to do and not a deterrent to their care if you just focus on the issue they’ve come to the ED to get treatment for.
On the military side of things, and having been in combat on the front lines, you don’t much care who is what – male or female – as long as they’re doing their jobs. When you’re fighting the enemy, you’re not taking an attendance check to see who’s showed up next to you to join in the fight – male, female, straight, gay, lesbian, bisexual, transgender – none of that matters. You engage your enemy with an application of force to make sure the enemy goes away and you remain living, breathing and standing. The readiness argument, in my opinion, is a bit of a red herring. You fight together. And you really don’t care whether it’s Bruce or Caitlyn Jenner fighting next to you as long as they’re engaged in the fight keeping your butt and their butt safe. When bullets are flying at you, you become instantly ready to apply lethal force, transgender or not.
At his confirmation hearing on Capitol Hill prior to his becoming President Trump’s Secretary of Defense, Gen. James “Mad Dog” Mattis was asked a question by Sen. Kirsten Gillibrand (D-N.Y.) pertinent to this debate. She asked of the general, “Do you believe that allowing LGBT Americans to serve in the military, or women in combat, is undermining our lethality?”
“Frankly senator,” Gen. Mattis replied, “I’ve never cared much about two consenting adults and who they go to bed with.”
“So… the answer is ‘no’?” asked Sen. Gillibrand.
“Senator, my concern is on the readiness of the force to fight, and to make certain that it’s at the top of its game,” he said. “So, when we go up against an enemy, the criteria for everything we do in the military up until that point when we put our young men and women across the line of departure, is that they will be at their most lethal stance.”
An important perspective to remember as this debate moves forward.
To learn more about Dr. Sudip Bose, MD, please go to SudipBose.com and visit his nonprofit TheBattleContinues.org where 100% of donations go directly to injured veterans.
It’s pretty rare that I see someone with symptoms like those of Arizona Sen. John McCain, who went into the hospital last week to have what his docs diagnosed as a blood clot above his left eye removed. It’s the same side of the senator’s face where he had several surgeries to remove patches of melanoma – a type of skin cancer that if not treated can be deadly. Sen. McCain had his melanoma taken care of and all was good. But his doctors were in for a surprise when they saw the blood clot and abnormal tissue above it. The lab confirmed what the doctors suspected and Sen. McCain learned not only did he have a blood clot, but he also had primary glioblastoma, a very aggressive type of brain cancer. It is the most recent blow to a man who has had a history stretching back some 50 years to the Vietnam War of having to fight through some very serious physical ailments.
It’s not often that I encounter a situation in the ER where I’m diagnosing a glioblastoma, but when I’m presented with a serious condition like that in the ER, it’s immediately humbling and I have instant empathy for the patient. It’s not easy to deliver a diagnosis like that. You want to be as positive as possible, but you also understand the reality of what your patient is facing. The statistics are daunting.
Glioblastoma, or GBM, tumors are usually highly malignant. The tumor cells usually reproduce very quickly and are fed by a large network of blood vessels. The American Brain Tumor Association says, “Because these tumors come from normal brain cells, it is easy for them to invade and live within normal brain tissue.”
Treatment can help, but the condition can’t be cured. Statistically, with this kind of tumor, survival rates beyond a year and a half are uncommon. Median survival time upon first diagnosis of GBM is in the 14- to 16-month range. There are some longer-term survivors, but this type of cancer is an aggressive form, and it’s usually more extensively present in the brain than the initial diagnosis indicates.
“I have no idea what I’m doing — I’m just a TV doctor … ”
— Alan Alda, from a health plan’s recent TV ad
Surely by now many have seen the advertisement using “TV doctors” from the shows, “Grey’s Anatomy,” “Scrubs” and of course “M*A*S*H*” to encourage everyone to have their annual physicals: TV Docs of America.
However, the president of the American College of Emergency Physicians (ACEP), Dr. Rebecca Parker, thinks that ad campaign was a waste of money. “The $9 million CIGNA spent on an ad starring well-loved actors playing physicians would have been better spent on patients,” she said. “Emergency physicians fight hard for their patients who are bearing an increasingly large share of the burden for their medical care,” she added. And therein lies the issue — increasingly patients find themselves caught between their health plans and their physicians. Emergency department (ED) physicians countered with their own video of real ED physicians as a parody of the CIGNA ad that included yours truly: ER Doctors of America – Parody of Cigna Health Insurance Ad (that’s me in the light-blue scrubs).
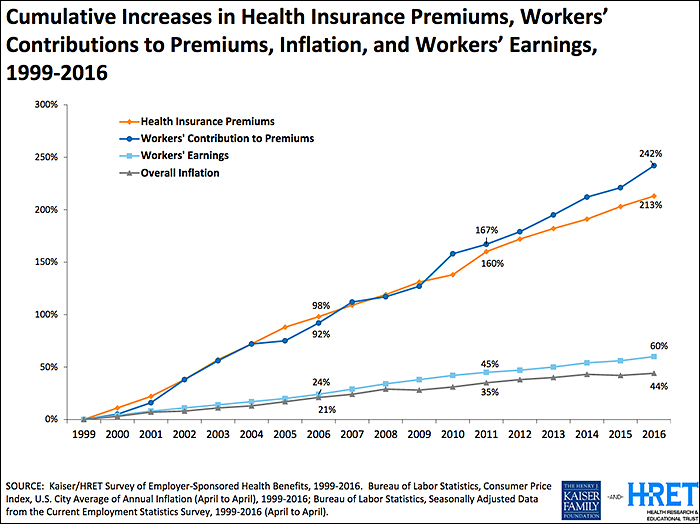
Twenty-plus years ago (when many of those TV doctors were in grammar school) the traditional employer-sponsored health plan was an “80/20” PPO plan (Preferred Provider Organization) where the health plan reimbursed 80 percent of the allowed physician charge and the patient reimbursed 20 percent (co-insurance) after his/her deductible. Unlike today, deductibles back then were perhaps as high as several hundred dollars but rarely in the thousands. Today the average individual deductible exceeds $1,400 according the Kaiser Family Foundation (KFF) and rose double digits just last year (see chart below). The patient has become the largest non-governmental payor in healthcare. Today what the average patient spends on deductibles (which is what a patient pays before their health insurance coverage kicks in), co-insurance and co-pays (patient cost sharing) is less than the average deductible, so the average patient is “underwater” even before insurance kicks in.
While the ACA (the Affordable Care Act, also known as Obamacare) did not create “high deductible health plans” (HDHPs), it certainly accelerated their growth and use among the millions who purchased the benchmark ACA Silver Plans. At above 250 percent of federal poverty level (FPL), folks who purchased Silver Plans have limited first-dollar coverage for preventative care and immunizations but faced HDHP features that many who obtained employer-sponsored coverage have experienced for many years. The net result of these trends and legislation meant that the patient became the largest non-governmental payor in healthcare — and many have experienced the “surprise coverage gaps” that were unheard of 20-plus years ago.
Emergency department (ED) access and treatment are mandated but reimbursement is not:
In 1986, Congress passed the “Emergency Medical Treatment Active Labor Act” or EMTALA, and as a result, the greatest unfunded mandate in healthcare in American history was launched. EMTALA mandated that every person who presented him or herself to an emergency department was entitled to a “medical screening exam” (MSE) and stabilizing care for an emergency. Hospitals are required to have specialty physicians “on call” – e.g. orthopedics, neurology, cardiology, surgery, etc. – so the MSE and stabilizing care could be completed. So health plans knew then and today that their members will not be turned away from the ED regardless of their insurance, deductibles or cost-sharing levels.
In 1997, Congress also enacted the “prudent lay person” amendments to the Balanced Budget Act of 1997 (BBA ’97) which required Medicare and Medicaid managed care plans to permit a person’s access to the ED if he/she believed, as “a prudent lay person”, that he/she was having an emergency including suffering from severe pain. BBA ’97 was essential, as prior to that law health plans were requiring that patients call and receive “prior authorization” for ED visits or the plan would retrospectively deny the ED visit for reimbursement. So while access (EMTALA) and treatment (BBA ’97) were guaranteed by federal law more than 20 years ago— unfortunately reimbursement for those mandated services was not itself mandated.
HDHPs and “the myth” of coverage—surprise coverage gaps are born:
Surprise coverage gaps occur when an ED patient reasonably believes that they are having an emergency, are treated by the ED and then discover after the fact that their health plan does not provide fair coverage for the services that were provided to them or their family member. One common coverage gap is that the patient’s health plan will reimburse the physician at or about Medicare levels—leaving a large “balance”, or difference, between that “allowable charge or rate” and the clinician’s charges or the “balance bill”, particularly where the clinicians were “out of network” (OON), which of course the patient has no control over.
The Medicare fee schedule is a creature of federal law and regulations and restricted by those laws in providing for fair coverage for services. In fact, comparing Medicare payments to inflation from 1992 to 2016, Medicare reimbursements have decreased over 50 percent. A non-profit Rand Study in 2016 found that nearly one-third of New Jersey hospitals would have net operating losses if reimbursement rates were at or near Medicare levels. So at a time when non-profit health plan executives are reaping millions in compensation—the top 10 executives at Health Care Service Corp. (owner of BCBS plans in Illinois, Montana, New Mexico, Oklahoma and Texas) split approximately $58 million in 2015 (see: Modern Healthcare Sept. 26, 2016) —they put profits above patients and stuck the patients in the middle of potential disputes with their physicians.
Hospital-based physicians lead the charge to remove the patients from reimbursement disputes:
National physician specialty organizations such as ACEP, the Anesthesia Society of America (ASA) and a healthcare trade organization, the Emergency Department Practice Management Association (EDPMA) recognized the need to do several things:
Establish a minimum benefit standard (MBS) that represents fair coverage for OON services and is transparent to the stakeholders
Remove the patient from the controversy between the physicians and health plans
Permit mediation of disputes between the plans and physicians that would efficiently address these issues
In 2015, ACEP and EDPMA formed a Joint Task Force (JTF) to develop strategies, white papers and documents to assist their members in addressing their state-level legislative issues. Based on the JTF’s 2016 Strategies White Paper, ACEP and ASA then wrote common principles and proposed solutions (some of which can be found here: ACEP Outlines Top Priorities for Replacing ACA), and now nearly 10 national medical societies have adopted their common sense solutions. An AMA resolution was pending for their June 2017 meeting.
A new non-profit, multi-specialty advocacy organization was born in 2016, Physicians for Fair Coverage, Ltd. (PFC). “The PFC immediately went to work to build on the ACEP/EDPMA JTF work and to write “model legislation” as the OON legislation issues were cropping up in nearly 15-20 states,” said Ed Gaines, an attorney with Zotec Partners, LLC, a large physician revenue cycle management company. Gaines also is chair of the ACEP/EDPMA JTF and serves as model legislation chair for PFC. “ACEP’s survey from February 2017 showed that 95 percent of patients want health plans to cover ED care, so we need to find a fair coverage, patient-centric and transparent solution to these issues,” Gaines said.
As a working ED physician, we see every day that there is a “cost/quality” equation playing out in our hospital EDs — and increasingly the unfunded mandates of well-intended laws from over 30 years ago are bringing the healthcare safety net to the breaking point. “Frequently ED physicians ask me why the health plans seem to be targeting them when the ED is approximately only two percent of the US healthcare expenditures — and I shrug and tell them, ‘because they can and they know their members will be treated by you regardless of their insurance,’ ” Gaines said. “It’s patently unfair for the plans to do this but the ‘House of Medicine’ is together now like never before and we will successfully advocate for fair coverage for the nation’s patients,” he said.
What’s happening is that patients don’t realize just how much healthcare costs are being shifted to them because they generally focus on premiums and either don’t recognize or sometimes even actively ignore these copays and deductibles thinking they’ll be healthy all year and won’t have to worry about those costs.
It’s not just Emergency Departments that are struggling with out of balance costs – it’s the patients across the entire spectrum of health care who are now struggling to shoulder the burden of the costs. Patients readily recognize premiums – the amount they have to pay each month for their healthcare coverage – and largely, they haven’t really felt a pinch there because premiums have risen slowly over the past 10 years. What people often don’t pay that close attention to, however, are the other two legs of costs associated with healthcare – copays and deductibles[DSB1] . A copay is the percentage a patient pays each time he or she sees a doctor. The deductible is how much a patient has to pay before the insurance kicks in. What’s happening is that patients don’t realize just how much healthcare costs are being shifted to them because they generally focus on premiums and either don’t recognize or sometimes even actively ignore these copays and deductibles thinking they’ll be healthy all year and won’t have to worry about those costs.
How patients are becoming self-insured
What we’re seeing now is that an average patient’s healthcare spend is less than the average deductible. The patient is becoming the largest payor in health care because they’re paying for everything and not reaching their maximum deductible. So patients need to pay attention to all costs – premiums, copays and deductibles, and not just premiums alone. Basically patients have become self-insured except in cases of major hospitalization. That’s something that most don’t realize. Companies sell high-deductible plans and people don’t realize they don’t really have coverage – they’ve got a relatively major up-front cost to pay before their insurance kicks in.
Says Dr. Parker, president of ACEP, “Many people don’t realize how little coverage they have until they need medical care — and then they are shocked at how little their insurance pays. Others are not seeking emergency care when they need it — and getting sicker — out of fear their visits won’t be covered.”
As Forbes noted in a 2015 article regarding the ACA: “Furthermore, the strong regulatory and political focus on keeping premiums from increasing ‘too much’ forced insurers to increase deductibles, to the point that most people with ACA plans will not be able to collect benefits, even after paying all the premiums.”
In other words, most people with ACA plans are in the same boat, having such a high deductibles that they are essentially self-insured, because they’ll be spending all their own money for healthcare coverage and will not see any money come their way in terms of compensation or reimbursement from their insurance plan.
A Business Insider story from September 2016 (Americans’ out-of-pocket healthcare costs are skyrocketing) reported on findings of the Kaiser Family Foundation, a nonpartisan think tank addressing health policy issues, when it released its 2016 annual Employer Health Benefits Survey. They examined the cost of insurance for Americans and found, as the publication Business Insider characterized it, both good and bad news. The good news was that “premium costs, the basic monthly payment to be covered, are growing at an incredibly slow rate compared with recent history. According to the Kaiser survey, average family premium costs increased just three percent between 2015 and 2016, to $18,412. This year’s low family premium increase is similar to last year’s (four percent) and reflects a significant slowdown over the past 15 years. … Since 2011, average family premiums have increased 20 percent, more slowly than the previous five years (31 percent increase from 2006 and 2011) and more slowly than the five years before that (63 percent from 2001 to 2006).”
But, Business Insider also noted in Kaiser’s findings that, “the main driver of the slowing in premiums, unfortunately, is the rise of high-deductible plans. … In 2016, 83 percent of workers have a deductible — an amount that they have to pay themselves for medical care before insurance covers it — with an average of $1,478. The average deductible for workers has gone up $486, or 49 percent, since 2011. Additionally, the survey found that 51 percent of workers have a deductible over $1,000 — the first time this has happened since the survey began in 1999.”
By comparison, workers’ wages increased 1.9 percent between April 2014 and April 2015, according to federal data analyzed by the report’s authors. Consumer prices declined 0.2 percent.
‘We’re seeing premiums rising at historically slow rates, which helps workers and employers alike, but it’s made possible in part by the more rapid rise in the deductibles workers must pay,” Drew Altman, CEO of Kaiser was quoted as saying.
A story in the Los Angeles Times quantified the point made by Altman and the Kaiser Foundation findings. “Over the past decade, the average deductible that workers must pay for medical care before their insurance kicks in has more than tripled from $303 in 2006 to $1,077 today [and up to $1478 in 2016 as seen in the chart above], according to the report from the nonprofit Kaiser Family Foundation and the Health Research & Educational Trust,” reporter Noam A. Levy wrote in 2015. “That is seven times faster than wages have risen in the same period.”
What that means is that for the first time in our nation’s history, patients have become the primary payor for their medical costs.
“It’s a quiet revolution,” Altman was quoted as saying in the LA Times story. “When deductibles are rising seven times faster than wages … it means that people can’t pay their rent. … They can’t buy their gas. They can’t eat.”
Unfortunately that’s not an exaggeration.
How did we get here?
The cost of healthcare has been growing rapidly for decades. History shows that our modern healthcare system really saw its genesis back in 1929 and 1930 with the emergence of what eventually would became a well-known health insurance company, especially in the 1950s and 60s – Blue Cross-BlueShield. In 1929, Blue Cross started out as a partnership between Baylor University hospital and financially struggling patients. It was the year of the start of the Great Depression with the crash of Wall Street and families trying to figure out how to get through it all. Blue Cross began as a plan to allow patients to pre-pay 50 cents a month, which would allow a person 21 days of hospitalization a year. The plan proved so popular that it grew quickly – from about 1,300 in its early years to about three million in 10 years.
In 1930, a group of physicians quickly adopted the Blue Cross idea when they saw the kind of success it was having and created Blue Shield, which developed a plan similar to the hospitalization plan of Blue Cross; but this partnership was between physicians and patients. Again, for a monthly fee, Blue Shield members gained access to physician services. This plan also proved extraordinarily popular.
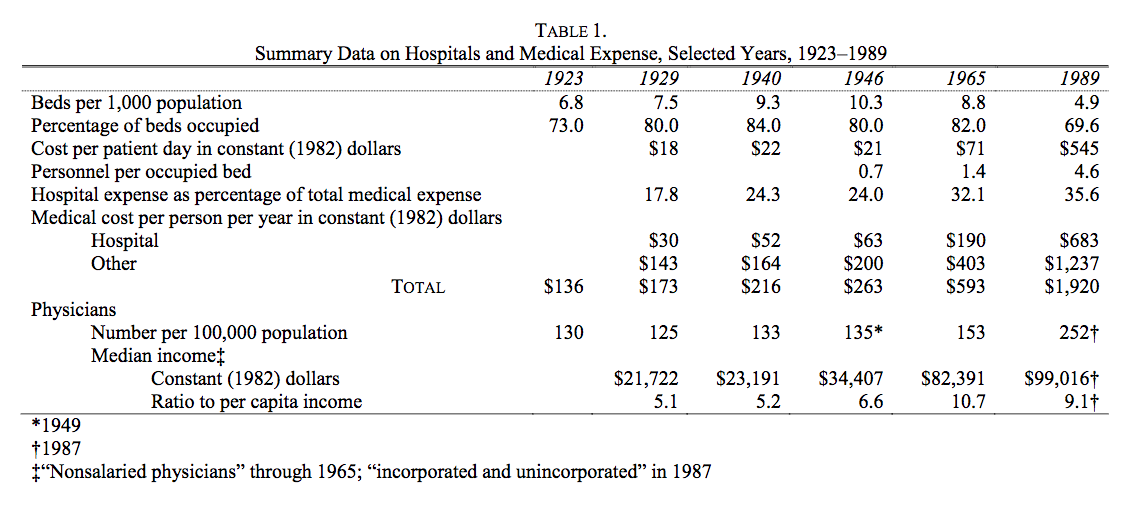
According to an often-cited and well-known study in healthcare circles by Milton Friedman published in 1992, “The cost of hospital care per resident of the United States, adjusted for inflation, rose from 1929 to 1940 at the rate of 5 percent per year; the number of occupied beds, at 2.4 percent a year (see Table 1 below). Cost per patient day, adjusted for inflation, rose only modestly.”
Moreover, according to Friedman’s research, The situation became very different after the end of World War II: “From 1946 to 1989 the number of beds per one thousand population fell by more than half; the occupancy rate, by an eighth. … [but] cost per patient day, adjusted for inflation, [rose] an astounding twenty-six-fold, from $21 in 1946 to $545 in 1989 at the 1982 price level. One major engine of these changes was the enactment of Medicare and Medicaid in 1965.” (My bold face highlight.)
The chart above accompanying Friedman’s research is particularly illuminating. A few highlights from Friedman’s study:
“Cost per patient day, which had already more than tripled from 1946 to 1965, multiplied a further eightfold after 1965.”
“Growing costs, in turn, led to more regulation of hospitals, further increasing administrative expense.”
“Anecdotal evidence suggests that increased administrative complexity played a major role in the explosion of total cost per patient day and led to a shift from hospital to outpatient care …”
And note in the chart above how much the total medical cost per person per year (in 1982 dollars) jumped from 1965, when Medicare was enacted, to 1989 – from $593 per person to $1,920.
“Even though more consumers are gaining health insurance coverage (from the mid-60s through the late 80s to modern day with the expansion of Medicare under Obamacare), they are by no means insulated from the burden of health care costs. Consumers are paying more of their health plan premium and experiencing higher out-of-pocket (OOP) cost-sharing for all types of health care services. These increases are expected to continue as employers shift to high-deductible offerings and individuals gain coverage through insurance marketplaces (also known as public health insurance exchanges).”
As physicians, we want fair insurance coverage for all patients to bring costs under control and have manageable coverage. Right now, not only are the costs not manageable, they’re often not even known by the patient.
Let’s say a patient comes through the ED and their costs are covered there, but then perhaps they get admitted to a surgical service and that assistant surgeon is out of network (OON), or a plastic surgeon comes in and sews up a laceration, and that plastic surgeon is not in network; the patient will get a “balance bill.” A balance bill is the difference between what the OON providers charge (let’s say that’s $1,000) and the amount reimbursed by the insurance carrier for that OON charge (let’s say that’s $450). So the patient’s left with having to pay $550, or the balance of the bill. The patients are then getting stuck with that bill, and that’s a problem.
It reminds me of an analogy I made in a previous write up (Obamacare: Three Keys for Improvement) where I compared insurance coverage to dining in a restaurant. I wrote:
“Have you ever been to a restaurant, paid what you thought was your bill, left, and then weeks later gotten a half-dozen or so bills in the mail related to your service at that restaurant? No? You say you haven’t? Perhaps you got a bill from the sous chef, who was an independent contractor not working directly for the restaurant? Maybe one from the food expediter, and then the one from the pastry chef, the maitre’d who escorted you to your table, the busboy who cleaned and set the table before you sat down and then cleared dishes after each course and filled water glasses? No? And just think — some of those people were in your preferred network of restaurant service providers (and you got a good deal on the cost of their services), but some weren’t (and you were charged what looks like an exorbitant amount).”
I’ll say it again: as physicians, we simply want fair insurance coverage for all patients. Insurance companies must provide fair coverage for their beneficiaries and be transparent about how they calculate payments. They need to pay reasonable charges, rather than setting arbitrary rates that don’t even cover the costs of care. Insurance companies are exploiting federal law [EMTALA] to reduce coverage for emergency care, knowing emergency departments have a federal mandate to care for all patients, regardless of their ability to pay.
As the president of ACEP, Dr. Parker, puts it: “Patients should not be punished financially for having emergencies or discouraged from seeking medical attention when they are sick or injured. No plan is affordable if it abandons you when you need it most.”
We all should be able to agree with that. And we all need to work together to get there. As I’ve written before, change has to focus on the center of the epicenter of healthcare — the doctor-patient relationship.
To learn more about Dr. Sudip Bose, MD, please go to SudipBose.com and visit his nonprofit TheBattleContinues.org where 100% of donations go directly to injured veterans.
Would you believe me if I told you that at a glance, I could predict your future health? No, I’m not an all-seeing or all-knowing deity of any sort, just a man armed with a medical degree and a heck of a lot of experience in battlefield operating rooms and in some extremely busy emergency rooms. I’ve seen things you wouldn’t want to see. I’ve seen dying and dead men and women, and I’ve seen, in quite a few cases, how they got into that state. I’ve seen their loving families sobbing with the loss of their loved ones. And all I’d have to do to make that determination is to take one look at someone’s body composition and the size of that patient’s waist.
If a patient was in the hospital because of issues related to heart disease or stroke or cancer or complications from diabetes, all I’d need to do is look at the patient’s waistline and I’d know the underlying cause without any blood work being done, or a CT scan or an MRI. I could tell you with certainty that obesity was a profound underlying cause of the state of ill health they’re in.
Medical school gave me a very fundamental lesson regarding body fat: Fat on the outside = fat on the inside (visceral fat), surrounding and choking internal organs. Obesity is the core element in many of the top 10 causes of death in the U.S. as listed by the Centers for Disease Control (CDC). And it’s an underlying cause in all of the diseases I just mentioned. That’s right – even cancer. Obesity increases levels of the hormones estrogen and insulin circulating in the body, which can stimulate cancer growth.
Obesity is the key element we need to focus on fixing as a nation to improve our overall health and longevity.
It’s certainly not easy to talk about death and dying in America. It’s immeasurably harder for one to go through a terminal illness.
Where there is life, there is death. It is inevitable for us all; yet as a society, we speak of it with hand over mouth – in hushed tones, as if the mere verbalization of it would bring it upon us. In America, we don’t deal with death very well. We want to believe that we will live to grow old and that death will be a quick and sudden event. That’s not always the case. It’s not a fun topic to talk about, and therefore we don’t talk about it nor do we plan for it properly.
We’ve got to get better about that. We’ve got to be open and honest about it. Because in the United States, we plan for death poorly or not at all. As an emergency physician, I’ve seen countless patients struck with a terminal illness, which has left families scrambling at the end of a loved one’s life trying to figure out what to do and struggling with life or death decisions. No one wants to feel like they have to step in and play God at that time. It puts family members in the position of trying to figure things out while they are in a highly emotional, stressed state. People usually don’t make the best decisions while distressed.
Family members often have a feeling of guilt if they haven’t discussed end-of-life care at some point, either before or during a terminal illness. They believe they should be doing everything possible to keep their loved one alive. But is that what the patient would want? Does it lead to a better quality of life? Is the patient unnecessarily suffering?
I once had a patient who had been declining in health for years. She was completely bedridden in her last days – couldn’t eat, go to the bathroom, etc. She was dying. It finally came to the point where she had to be put on a bipap air flow machine to keep her alive. The family knew that they didn’t want to put her on a ventilator, and they knew that if they removed the bipap machine, she wouldn’t survive. However, with a bipap machine, a patient can typically only go a maximum of about five days because it provides too much pressure and would cause damage to the patient’s face. The woman’s family ended up keeping her on the machine for the maximum amount of days. Understandably, it was difficult for the family to ultimately let their loved one go. But did it do much for the patient to lie there with a bipap mask on for the full five days? Was she just suffering even more by keeping the mask on? Were hospital resources used unnecessarily? Is that what the patient really would have wanted?
We should make an effort to talk about possible end-of-life decisions or scenarios with our loved ones. We should talk about and understand how each of the following items could play a role as a person approaches death:
Will
Living Will
DNR
Power of Attorney
Short-term Care
Long-term Care
Life Insurance
Trust
Financials
Also in the context of dying and end-of-life choices, we need to talk about the subject of palliative care and get comfortable with that concept. Palliative care is defined as the act of giving medical care to someone with a serious illness without actually dealing with the cause of the condition. It’s care that’s intended to alleviate a patient’s symptoms with the goal of improving quality of life, and often is associated with relief from pain. Yet all too often in America when palliative care is mentioned as a way to ease a person’s descent into death, we use those words almost euphemistically – we use the words “palliative care” as code words for death.
I’m not talking about actively hastening a patient’s death, I’m talking about giving a patient the highest quality of life possible as he or she faces a terminal illness. In the truest sense, palliative care is appropriate at any stage of a serious illness, absolutely can work in conjunction with curative treatment and should not ever hasten death.
Affirms life and regards dying as a normal process;
Intends neither to hasten or postpone death;
Offers a support system to help patients live as actively as possible until death;
Offers a support system to help the family cope during the patient’s illness and in their own bereavement;
Will enhance quality of life, and may also positively influence the course of illness;
Is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.
I heard something recently that caught my attention. It was in the trailer for the soon-to-be-released documentary film, “Eating You Alive.” The quote came from Randy Titony, a self-described plant-based evangelist who is certified in plant-based nutrition and also is a physical therapist professional. He said, “People aren’t living longer; they’re dying longer.”
That struck me as a very interesting perspective.
If you talk to a hospital administrator or any politician in about dying in America, they might point out that a full quarter of traditional Medicare spending is provided to beneficiaries in the last year of life. They might note data that shows that spending for this cohort is four times higher for those who died at some point during the year compared to those who lived the entire year. And they’ll very likely talk about unnecessary care and overtreatment. Yet time and again, attempts to roll back such “aggressive” care are thwarted by talk of death panels and accusations of rationing care.
According to Dr. Jordan Grumet, a leading palliative care specialist and hospice medical director in Northbrook, Ill., who also writes on the subject, dying has become miserable because we eschew dignity and turn it into a high-tech, costly, drawn-out, process.
As Grumet sees it, focusing on finances is misplaced. “Improving the end of life experience is bound to fail if we focus on finances,” he said. “No one wants to feel like they are dying on the cheap.”
Instead, he believes we need to concentrate on the concept of dignity. In short, he thinks we need to die better.
I would agree. Time and again I’ve seen people unprepared for death – patient and family alike – and unprepared even for its approach and the management of issues associated with that.
A recent study by Singer et al in The Annals of Internal Medicine found that the number of people experiencing pain in the last year of life actually increased by nearly 12 percent from 1998 to 2010. And the number of people with depression increased by 26 percent.
If we focus on high-quality interventions at the end of life, things like aggressive pain control, counseling, and symptom management, and at the same time minimize low-yield treatments that increase pain and suffering – like surgery and chemotherapy, for example – could we affect and reverse those trends cited in the previous paragraph? Things like surgery, chemotherapy, diagnostic imaging ― although often utilized during the last months of life ― infrequently improve outcomes and can prolong discomfort. This should be a process of shared decision making with the family and loved ones.
The result of this sort of treatment flip, if you will, would be that patients embrace and even enjoy the last stages of life. Says Grumet: “We help them die with the same dignity that they strove to live … and, believe it or not, that might actually save our health care system some money.”
It might even have a positive effect on the course of a patient’s illness.
Palliative care providers agree. Financial concerns are very real and no one wants to make decisions based on money as someone’s life appears to be slipping away. But with the medical system’s focus on treatments regardless of cost (driven largely by medical malpractice and legal concerns) coupled with the lack of discussion families have around end-of-life issues, patients and families alike frequently do not get the kind of care they hope to get.
In an article published in 2012, Money magazine quotes Ira Byock, director of palliative medicine at Dartmouth-Hitchcock Medical Center and author of “The Best Care Possible”:
“When patients have a terminal illness, at some point more disease treatment does not equal better care.”
The key is for families to discuss end of life issues and keep communication open with their loved ones going through it. In my career, it’s been interesting to watch how people handle the end of life process – when they have any control over it. I’ve known a man in his mid-80s who was battling Parkinson’s disease who made the decision that he was ready to die. Despite the efforts of medical personnel and family members, he suddenly refused to eat, drink or take any medication. He couldn’t speak, but he knew what he was doing and family members came to understand that. He died within a day and a half.
Others will desperately cling to life, not wanting to go – hanging on without food or water for days and weeks. The importance of the possibility of one more day seeing a father, a mother, another day seeing a brother, a sister, a grandson, a son or daughter, might suddenly become a reason for living — a very powerful reason for fighting for life.
A study done by Diane E. Meier, Director of the Center to Advance Palliative Care, Professor of Geriatrics and Palliative Medicine at the Icahn School of Medicine at Mount Sinai, published in September 2011 in the Milbank Quarterly, reported the following in her findings: “Palliative care and hospice services improve patient-centered outcomes such as pain, depression, and other symptoms; patient and family satisfaction; and the receipt of care in the place that the patient chooses. Some data suggest that, compared with the usual care, palliative care prolongs life. By helping patients get the care they need to avoid unnecessary emergency department and hospital stays and shifting the focus of care to the home or community, palliative care and hospice reduce health care spending for America’s sickest and most costly patient populations.”
It’s amazing how precious life is, and how much you will fight to hold on to it when the fight is still in you, and how quickly it can go when there’s no fight left. Every patient, family, case and doctor is different. The key thing is to get education around palliative care and end of life care, have open and frank discussions, and memorialize your decisions and preferences in medical records and documents such as a living will, for example, and make sure your doctors and other care providers know what your wishes are.
From the previously cited Money magazine article: “A 2010 study in the Journal of Palliative Medicine found that only 15 to 22 percent of seriously ill elderly patients had their preferences in their medical records.” And, “studies by the Agency for Healthcare Research and Quality show that 65 to 76 percent of doctors whose patients had documents outlining end-of-life wishes weren’t aware they existed.”
Families need to engage amongst themselves and with their care providers in advance about the implementation – or not – regarding palliative care. It’s not only a treatment and financial decision, but a quality of life decision as well.
To learn more about Dr. Sudip Bose, MD, please go to SudipBose.com and visit his nonprofit TheBattleContinues.org where 100% of donations go directly to injured veterans.
Our country has to maintain a strategy to use against a potential microbial attack that would strike terror in the hearts of every American if we’re not prepared for it when it hits. And make no mistake, it will come. It’s only a question of when.
Are we ready for the next pandemic? I would say no. We’ve made a start in preparing, but we’re not ready for a full-on microbial assault by any stretch.
“Pathogens with pandemic potential continue to emerge, and most of them are of animal origin (zoonotic). They include, for example, Ebola, H5N1 avian flu, H7N9 avian flu, HIV/AIDS, and two kinds of coronavirus: severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome (MERS).”
The World Bank also points out that that:
“The 1918 pandemic flu, the most severe of the four flu pandemics in the last 100 years, infected up to 40 percent of some national populations and killed 50–100 million people.”
Let’s start at the beginning: a pandemic is an epidemic of infectious disease that spreads through human populations across a large region – a country or countries, a continent, or even worldwide ― usually resulting in health issues serious enough to cause massive death among those infected.
“If anything kills over 10 million people in the next few decades, it’s most likely to be a highly infectious virus rather than a war. Not missiles, but microbes.”
That’s a quote from a TED Talk given by Microsoft co-founder Bill Gates in early 2015, only about a year after the start of an Ebola outbreak in West Africa, which ultimately claimed almost 29,000 lives. It’s now two years later, and the warning Gates gave still rings true as a very valid concern. In his talk, he said that there was no need to panic about this, but that, as a country, “we need to get going.”
He may have been right about not needing to panic. But it’s time to get going now.
The big question, though, is how? What do we do? How do we prepare for something that is ultimately unknowable until it hits?
We have a fairly recent example of a viral outbreak that can help us get ready for that fight – the Ebola virus outbreak in West Africa of just a few years ago that I just mentioned. It was an unprecedented epidemic with an unprecedented response that took years to get under control. The independent medical humanitarian organization, Medecins Sans Frontieres (MSF) – more widely known in the U.S. as Doctors Without Borders – organized a global response to the outbreak. The group is primarily made up of doctors who volunteer their time and expertise to any given global medical threat.
At its peak, MSF employed nearly 4,000 national staff and over 325 expatriate staff to combat the epidemic across the three countries.
In Liberia – just one of the three primary countries where the Ebola outbreak extended to – 189 health care workers died after contracting the virus. That’s one of every 10 workers who dedicated themselves to stopping the spread of the outbreak. Unfortunately, that pales in comparison to the general mortality numbers of the outbreak, which show that of the total 28,636 documented cases of people infected by the Ebola virus between 2014 and January 2016, there was a resulting 11,315 deaths, according to the World Health Organization (WHO). That’s a mortality rate of nearly 40 percent. Very scary stuff.
According to the non-fiction book, The Hot Zone, written by Richard Preston and published in the mid-’90s after the Ebola virus first emerged from the jungles of Africa and claimed its first human victim, Preston writes:
“A hot virus from the rain forest lives within a twenty-four-hour plane flight from every city on earth. All of the earth’s cities are connected by a web of airline routes. The web is a network. Once a virus hits the net, it can shoot anywhere in a day – Paris, Tokyo, New York, Los Angeles ― wherever planes fly. Charles Monet and the life form inside him had entered the net.”
Charles Monet was the man initially infected with that life form – the Ebola virus ― who Preston was writing about in The Hot Zone. Monet was trying to get to a hospital in Nairobi, Kenya, flying aboard a Kenya Airways flight. It was nothing more than luck that Monet didn’t infect anyone on the plane and luck that the virus really didn’t “enter the net” and spread worldwide. And this was some 35 years before the Ebola outbreak in 2014.
The next big viral outbreak doesn’t necessarily have to be something as exotic as an Ebola virus or some other as yet unknown zoonotic pathogen. It could simply be the next strain of influenza – the flu – that we’ve never seen before that could turn deadly. The source could be a natural epidemic, or it could be bio-terrorism.
Here are some of the steps we need to take to avoid at least a major worldwide health scare or at worst a pandemic:
Speed is the first factor. We’ve got to be able to quickly identify the threat and move to treat it as fast as possible. Speed is the ultimate weapon. Identification usually the easy part. Then what, though? How do we minimize the spread of the infection and contain it?
Reserves – in a word – just as in we have now as part of our current military. We need medical reservists who can be called up to handle an infectious outbreak – a U.S. medical dream team ready to be deployed to the hot spots and begin front-line treatment and containment.
We need a group of key epidemiologists also ready to evaluate the disease and formulate a plan for the most effective treatment of the “microbial missile.” We need dedicated researchers who can identify and formulate treatment protocols, develop vaccines and research the most effective ways to eliminate the threat. Modern advances in biology should lessen the turnaround in the time it takes to look at a pathogen and then find a quick path to manufacturing drugs and vaccines at scale that could work against that pathogen or develop a universal treatment protocol to be implemented.
Exercises – practice. Now is the time to identify the personnel who would make up these teams and train them. We need to perform military-like exercises – “germ games” as Bill Gates called them in his TED Talk – to be ready for an outbreak. We’ve invested a lot as a nation to build up our military defenses – people, weapons and weapons platforms, hardware, software, logistics, networks, command structure – all of it. But if the next big threat to US human lives is microbial, what do we have invested right now to stop a major epidemic? Very little.
So we’ve got to get a response team ready. We’ve got to get a preparedness team ready to roll.
WHO is funded to monitor epidemics, but not to take action to stop them. We can’t let that gap go unfilled here in America.
The World Bank estimates that if we have a worldwide flu epidemic, we’d have millions of deaths. And they also say that as a result of the epidemic, global wealth would depreciate by more than $3 trillion. Not million, not billion – trillion.
Invest now. If we invested even a small fraction of that astronomical amount of money in readying to stop such an outbreak, wouldn’t it be worth it? And this kind of investment would evolve significant benefits beyond just being ready for the next pandemic. This should absolutely be a priority. We can build a terrific response system.
Leverage technology. Technology is advancing at such a rapid pace that we’re barely able to keep up with and implement the improvements made on a monthly and yearly basis. So who knows the kind of technology we’d be able to leverage in the future. But even so, currently we can use modern technology that is now as simple and basic as cell phones. Cell phones can get information fed in from the public and can also be used to get information back out instantaneously. Satellite tracking can monitor people movement.
Response. Why not pair the medical people with the military to take advantage of the military’s ability to move quickly in response to a threat? It’s an idea Bill Gates surfaced in his talk, and I would agree with the strategy. There’s not one area of America we couldn’t get to quickly if we paired up the medical personnel with military movement and transportation.
There is a lot of room for progress and a lot we can do to be ready for the next pandemic. And we need to start now.
To learn more about Dr. Sudip Bose, MD, please go to SudipBose.com and visit his nonprofit TheBattleContinues.org where 100% of donations go directly to injured veterans.
All that the doctors who treated Cincinnati, Ohio resident Otto Warmbier knew is what they had seen or maybe read in the news. They knew he had just been released on June 13 from imprisonment in North Korea where he had been held by for more than 17 months. He had been sentenced in March 2016 to 15 years of hard labor for allegedly removing a propaganda poster from a wall at a Pyongyang hotel where he had been staying. The University of Virginia honors student had been visiting the authoritarian state during a five-day trip with a group called Young Pioneer Tours, which is a group out of China – an important note.
Otto Warmbier (Facebook)Otto Warmbier’s ordeal began on Jan. 2, 2016 when he was removed from a flight that was about to leave Pyongyang, the capital of North Korea, by two North Korean officials who explained that he was very sick and needed to go to a hospital. He was not sick and did not need to go to a hospital. He had just been arrested for allegedly trying to steal that poster.
Most of us have seen the video by now of Otto Warmbier in captivity from March 2016 – just a couple months after he was removed from the flight – he was alert and made a confessional statement in front of media cameras, where he pleaded for leniency and then broke down crying. In another video clip, we see him paraded before cameras being roughly escorted by two North Korean soldiers who had tight grips on each of his arms, his head bowed, his feet shuffling.
Then came the news well over a year later that through various means of diplomacy, he was being released to go back home to Cincinnati, but that he was in a coma and had been for most of his time in captivity. The explanation from the North Koreans? He had contracted botulism and had taken a sleeping pill.
Cutting back on sugar will do more than shrink your midsection, it could save your life. Overindulging on sugar is a major contributing factor to the obesity epidemic. The connection between the rise in sugar in our diets and both illness and death is not coincidental. Some known side effects of overindulging on sugar are metabolic disease, type 2 diabetes, liver damage, fatty liver, abdominal obesity, high cholesterol, certain cancers, increased triglycerides, heart disease, tooth decay, increased cravings, mood swings, attention deficit disorder, skin issues, acidity and a lengthy list of list additional physical, emotional and mental ailments.
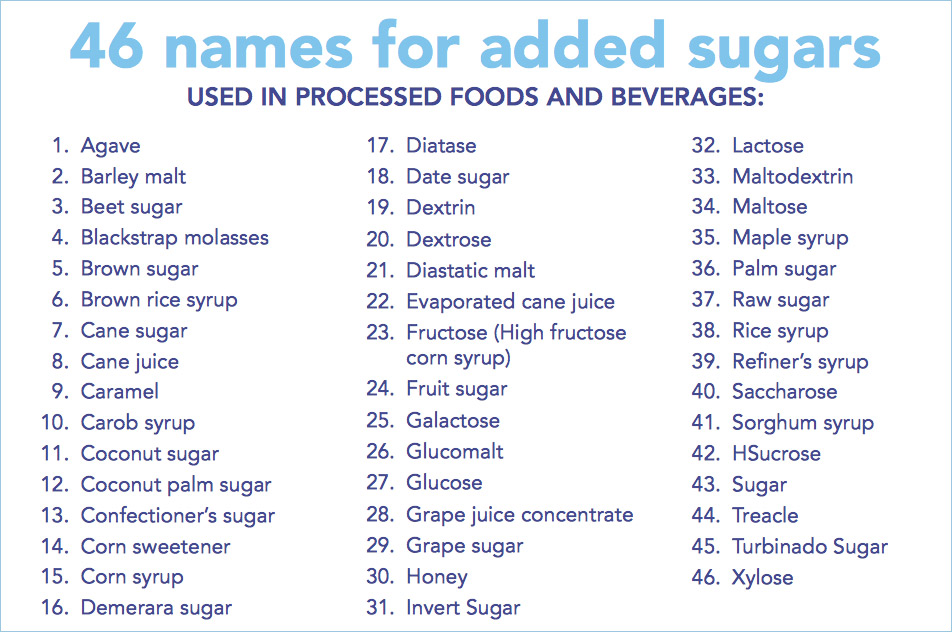
The consumption of fructose has increased by 600 percent in the past 25 years. Six hundred percent! If you were to remove all of the foods from the grocery store that did not contain added sugar, only 20 percent of the items would remain. The tricky part is that sugar is delivered to you in packaged products disguised by dozens of different names, from inulin to molasses, to agave nectar to maltose and diatase and the more well known high-fructose corn syrup.
The average American consumes 40 teaspoons of sugar a day. Your health in large part depends on what you buy at the store.
Kelli Calabrese, a Clinical Exercise Physiologist and Certified Nutrition Specialist, suggests that cutting out the obvious sugars such as candy, cake, diet soda, processed foods and desserts are a good place to start; however, sugar is hidden in places you might least expect it. Become a label reader and you will be surprised at the quantity of sugar in foods from ketchup and barbeque sauce to yogurt and orange juice. Even if you are young, lean and healthy you should minimally consume foods with added sugar. If you are overweight, added sugar should be avoided. Sugar doesn’t add any physiological benefit, can damage your metabolism and actually can take resources from your body to process.
There are many reasons why emergency rooms are dangerously overcrowded. With millions of Americans lacking adequate access to primary care providers, emergency rooms have become the primary health care system and safety net for the uninsured, underinsured and those without access to other medical care. Overcrowded and with overworked staffs, ERs are perilously close to collapse in many places. (See my other article on ERs here: Our Nation’s Emergency Rooms). In fact, many already have closed their doors. There is an increased demand for emergency department care, as hospital emergency rooms have experienced a 32 percent increase in patient volume over the past decade.
There are many reasons why we are seeing an influx in the volume of people seeking care in the ER. For starters, the fastest-growing age group in the United States is those over age 65, according to the 2010 US Census, and emergency room visits by the elderly are rising at an alarming rate. We also have a shortage of primary care physicians, and a growing percentage of health care practitioners that do not accept Medicare and Medicaid because of low reimbursement rates. Confounding those issues is the EMTALA (Emergency Medical Treatment and Active Labor Act) of 1986, which requires emergency rooms to treat all comers, regardless of urgency or income. Two-thirds of emergency visits occur after business hours, when doctors’ offices are closed. For people who find themselves in distress without access to care for these various reasons, the emergency room is often the only place to turn, and the double doors will always be open for them.